What is it?
Simply, the most common use for spirometry is to measure how much air we can breath out in 1 second (FeV1) and how much we can breathe out total (FVC).
For myself and my clients, I use a Mir Spirobank Smart.

The test is done by taking a deep breathe in, placing your mouth around the tube, then blowing as long and hard as possible. Typically, I’ll do this 3 times, both to give the client a little bit of practice with the device and to get an average idea of performance.
Assessment
After this, I take FeV1 and FVC and compare it to data by the Global Lung Function Initiative (GLFI). This then compares my client against what is average on the combination of age, height, sex, and race. This data is also continually updated with ongoing research, and with time has been adding more options in the selection of ‘race’.
For the example case I am reviewing, I will be showing my own data.
Male, 175cm, male, Caucasian
Predicted
(measured in litres)
Compared to average, I am happy with these results.
Issues with Limitations
If a client shows a number below average, this is a red flag both for their health as well as their ability to progress in exercise.
Concern #1
Effect of respiratory illness: a below average lung function means an increased amount of dead space in the lung, for which any additional limitation increases the danger to the individual. Dead space is the air that does not get exchanged on each breath, but only the air that goes in and out on each breath. All remaining air is considered that dead space.
With a respiratory illness, we can divide between the upper and lower respiratory tracts. The upper is the nose, nasal cavity, mouth, and throat. The lower respiratory tract is the windpipe and everything in the lungs. An upper respiratory restriction means either increased effort to breathe through the nose, and/or breathing through the mouth, which comes with its own issues. A lower respiratory limitation means there is less surface area of the lungs to be able to take in oxygen, in turn increasing risk of hypoxia (low oxygen in blood).
A low spirometry score means that any additional limitation increases the risk of harmful outcomes form respiratory illness due to the body’s inability to supply enough oxygen to the body.
Concern #2
Exercise performance: when we exercise, our body has to manage how its chemistry changes from the work we are doing. The harder we work, the more CO2 our bodies generate and need to blow off to manage our ph, which wants to be between 7.35-7.45 (slightly alkaline). Anaerobic exercise (burning carbs/sugars without O2) increases the acidity of the body, a cycle which is addressed ultimately by blowing off CO2 when we breathe faster and/or deeper.
A person with a below average FeV1 will struggle to have each exhale be big enough to off-load enough CO2 to prevent the body from becoming too acidic. In this case, the person will always find that their exercise is limited because their muscles are burning too much to continue. This can be deceptive as to the problem, because the person cannot breathe fast or hard enough to ever feel their breathing tire out. Concisely, this is a breathing limitation disguised as a muscle limitation. It is easily identified if spirometry is tested.
How to Improve
As with all training, measuring is necessary to assess if there is an improvement.
Spirometry itself is a tool for measuring, not for training.
Training can be applied either with a respiratory trainer or through exercise.
A respiratory trainer involves an app-connected device to give feedback on both the speed and volume of the breathing, done for time. It prevents hyperventilation by controlling how much CO2 the person breathes back in, so clearly a case of science = magic!
To apply this in exercise, a further assessment is necessary with a metabolic cart. This can then identify at which heart rate the person starts struggling to breathe in activity, either by volume or speed. Interval training can then be assigned so the person can specifically train where they struggle.
Seeing Results
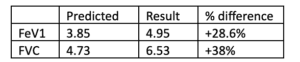
For myself, I did 12 weeks of interval training based on the HR where I struggled to breathe obtained from the metabolic cart.
This is the results:

This is a significant improvement obtained through doing specific training 1x/week. I do not know what my upper potential is, but I do know that I am closer to it, and my body benefits from improving my ability to breathe.
Need for Normative Data
Spirometry is a simple thing to measure, just blow into a tube. The value to knowing how strong your lungs are is immense. While everyone can work to improve, this is potentially critical information for anyone who is below average. Any health issue involving breathing is of increased risk of requiring medical intervention if the lungs are too weak to keep up with the person’s need of oxygen. Training respiratory function is a straight forward method to stack the deck in one’s own favour, and that is a value that can’t be measured.
Additionally for athletes after a respiratory illness or other limitation, prior data is necessary for the athlete to know if they are recovered or not. It is possible that the athlete could still score above average for FeV1 and FVC, but this could still be a significant limitation in performance. This can only be identified if prior ability is assessed.
If you have any further questions about spirometry contact me here email me at David@IntegratedStrength.ca

